Archive
-
Challenging the Status Quo for Youth Mental Health
Comments Off on Challenging the Status Quo for Youth Mental HealthThe headlines have been filled recently with the tragic news of young Canadians taking their own lives, serving to highlight a pressing issue that must be addressed: the need to provide youth with the help they need in order to prevent dire consequences like suicide.
-
What does Education have to do with the Mental Health of Children and Youth?
Comments Off on What does Education have to do with the Mental Health of Children and Youth?There is a clear and well-researched relationship between student mental health problems and academic difficulties. When students are preoccupied with emotional concerns they cannot participate fully in learning. Also, students who are experiencing academic challenges due to learning disabilities, intellectual disabilities, or other learning challenges can develop mental health problems, such as anxiety or depression. These concerns also interfere with social relationships and contribute to feelings of low self-worth, anger, worry and confusion. Since mental health problems are often difficult to treat, the earlier the intervention, the better the trajectory for a student vulnerable to mental illness.
Fortunately, there is now a significant body of research that shows there are programs and practices that can be used to support children and youth at risk. These programs can keep students from falling into a negative spiral by bolstering social, academic, or emotional skills, changing negative thought patterns, and nurturing a sense of well-being. As well, psychosocial treatments, like cognitive-behaviour therapy and parent training, have been proven to be effective in helping students with anxiety, depressed mood, and behaviour problems. The use of medication has also been shown to be helpful for some children and youth struggling with particular mental health problems. Even when difficulties are long-standing, there are ways to help students and families to effectively manage the disorder, just as you might with other chronic health conditions.
Since mental health problems are often difficult to treat, the earlier the intervention, the better the trajectory for a student vulnerable to mental illness.
Unfortunately, very few children and youth who struggle with mental health problems will access the help they need. There are currently several barriers to getting help:
- Often the stigma associated with acknowledging emotional problems prevents many people from accessing services.
- Caring adults and peers may be in a position to help, but they often feel ill-equipped to identify problems and to know where to find professional assistance.
- Finally, even when problems are voiced and/ or identified, in some communities there are not enough services to meet the demand.
Since every child is required to attend school, these issues with access make schools an important place to support students with mental health concerns. Indeed, schools are an optimal setting:
- to reduce stigma;
- to promote positive mental health;
- to build student social-emotional learning skills;
- to prevent the development of mental health problems in high risk groups;
- to identify students in need, and to support them in accessing community services.
It is very important that teachers and support staff understand that they are not expected to become counsellors or therapists nor are school boards expected to do the work of community mental health organizations. Rather, what is important is that education has a role to play in a full system of care. This role involves creating caring schools and classrooms, building social emotional learning skills, and helping to identify students in need of early intervention.
Adapted from: Leading Mentally Healthy Schools: A Resource for School Administrators (School Mental Health – ASSIST, 2013)
This blog post is part of CEA’s focus on student mental health, which is also connected to Education Canada Magazine’s student mental health theme issue and a Facts on Education fact sheet on what the research says about effective approaches to improving students’ mental well-being. Please contact info@cea-ace.ca if you would like to contribute a blog post to this series.
-
What is Student Anxiety?
Comments Off on What is Student Anxiety?Anxiety is a typical part of growing up. In fact, it is a normal reaction to stress. For most kids, feelings of anxiety and fear come and go. Most developmental phases lessen and disappear over time. Examples of normal developmental fears in infants and toddlers include separation from parents or sudden and loud noises. Preschoolers may be afraid of dark environments or animals. Children in primary and junior grades may worry about performance or bodily injury. Those in intermediate grades may begin to experience stress related to their health and appearance. In high school, anxiety may be related to school performance, social belonging and the future.
An exaggerated experience of thoughts, feelings, behaviour and sensations associated with stressful life events that interfere with functioning and/or cause distress is an indication that the person is overestimating the threat and underestimating their ability to cope. When anxiety overtakes the person’s ability to think rationally, it affects their ability to move forward. This is when teachers need to be concerned about students.
Everyone gets anxious at one time or another. Stress is normal and can be adaptive. Anxiety, however, may be observed in an exaggerated fear response, which means becoming fearful in a situation that is not dangerous. For example, you might feel anxious about learning to drive a car. As such, you might practice with someone you trust, drive slowly and be selective on the roads you choose. However, when feelings of anxiety occur persistently over longer periods, without appropriate reason or are exaggerated, the anxiety can become debilitating.
Fear is experienced when one actually faces danger. That is an example of an adaptive fight or flight response. When a person experiences high levels of anxiety with no real danger present, this is when anxiety may become debilitative based on the misperception of a threat.
Some anxiety is helpful because it keeps us cautious, safe and performing well. When a situation is anxiety provoking, if a person can harness the positive, the anxiety is not harmful to them and may actually motivate them to face the challenge.
An exaggerated experience of thoughts, feelings, behaviour and sensations associated with stressful life events that interfere with functioning and/or cause distress is an indication that the person is overestimating the threat and underestimating their ability to cope. When anxiety overtakes the person’s ability to think rationally, it affects their ability to move forward. This is when teachers need to be concerned about students.
When is anxiety a problem?
The flight or fight response is adaptive when facing danger. However, when the danger has passed or there is no real danger, a flight response (avoidance) or a fight response, (aggression) is maladaptive. Furthermore, if a person persistently experiences high levels of anxiety although no real danger is present, the anxiety becomes debilitative.
Most normal anxiety is short-lived. Anxiety may be a problem for students when:
- it is very intense;
- it is unreasonable or out of proportion to the situation;
- it persists over longer periods of time; and/or
- it interferes with their ability to learn, socialize and participate in activities.
If you are seeing these concerning signs, this is the time for you to seek the support of the mental health professionals in your school board or community. Professional support is important because the earlier we intervene, the sooner we can help. Early intervention can teach life-long skills for managing anxiety. There is effective treatment for anxiety disorders.
Adapted from SMH-ASSIST Anxiety Module, 2014
This blog post is part of CEA’s focus on student mental health, which is also connected to Education Canada Magazine’s student mental health theme issue and a Facts on Education fact sheet on what the research says about effective approaches to improving students’ mental well-being. Please contact info@cea-ace.ca if you would like to contribute a blog post to this series.
-
Creating an Ethos of Care in our Secondary Schools
Comments Off on Creating an Ethos of Care in our Secondary SchoolsRelationships, relationships, relationships! It sounds cliché but in fact this is the heart of the matter. Every student has a story and the story is crucial to his or her sense of well-being. It seems easier, more manageable to know the “stories” of our students in the earlier grades. One teacher and one group of classmates equal a family. Where we seem to have more difficulty navigating the storyline is in our secondary schools. Students have many teachers, many sets of classmates, changes throughout the year and from year to year.
Our school is the hub of the community. It is a safe place for students to reveal their story. There are professionals who care. Our teachers want to make a positive difference in the lives of students. However, teachers cannot do this work in isolation. It is crucial to develop practical systems that support their work. They want to impact society and prepare the minds of the future. Where the tension exists is when dealing with matters of the heart, the emotions? This was previously the responsibility of the parents. These were discussions that lived privately within the confines of the family. This has evolved and these conversations are presenting in our schools.
How do we foster an ethos of care in our school that extends beyond the confines of academics? As a school community we have been compelled to answer some hard and challenging questions. How we effectively equip our teachers to deal with students who are struggling? Do we know the true reasons why students are not succeeding? Is it intellect, effort, a lack of support or is it our systems and school culture that need transforming? Do we believe that all students deserve to experience success? How do we define success for our students? Are we just committed to preparing students for the future, for their “real life”? Can we agree that their real life is right now and are we able to assist our students in building their own positive futures? Are we willing to listen to the “stories” of our students and respond appropriately?
Where the tension exists is when dealing with matters of the heart, the emotions? This was previously the responsibility of the parents. These were discussions that lived privately within the confines of the family. This has evolved and these conversations are presenting in our schools.
These challenging questions are at the heart of many robust conversations amongst our staff. The discussions take time and do not happen overnight. There are implications for scheduling, teacher assignments, and the allocation of resources. Most importantly, what success indicators we will accept that we are moving in the right direction as a school and how we will celebrate the successes.
We agree that the most vulnerable times for students are when they experience transition. We have decided to get to know our students prior to them arriving at our door. We begin to work with our feeder schools as early as possible. We identify students who might be experiencing difficulties in their school and family lives. We put our energy into transitioning all students and do not just make room for the “good” ones.
We endeavor to ensure that there is one adult who knows the story of every child in our school community. Each teacher chooses a student to put some extra energy into, to find out his or her story. Teachers agree to document what works and even more importantly what fails. They agree to share this information with their colleagues on a consistent basis.
We have established a Mental Health program in our school. We have 4 youth support workers who act as mentors to students with mental health challenges. We discovered we were losing Grade 10s in their first semester of high school. We have our youth workers spend time in our feeder schools getting to know the Grade 9s. Their purpose is to build relationships and begin the conversations about successfully transitioning to high school.
We invite all of our Grade 9 students who present as having challenges to join us in summer programming prior to their Grade 10 year. We offer two courses that are required for a high school diploma. We staff these courses with “rock star” teachers. These students earn credits for two courses, they get to know us with a smaller student body, they become familiar with the school and our culture of high expectations and they don’t spend the summer worrying about the transition.
We want to debunk the myth that students will be “on their own” once they get to high school. We have built support systems for our teachers and their charges. Getting to know the stories of our students is the only way to begin to deal with the “health” of our school!
This blog post is part of CEA’s focus on student mental health, which is also connected to Education Canada Magazine’s student mental health theme issue and a Facts on Education fact sheet on what the research says about effective approaches to improving students’ mental well-being. Please contact info@cea-ace.ca if you would like to contribute a blog post to this series.
-
What on Earth are EBPs and EIPs?
Comments Off on What on Earth are EBPs and EIPs?The terms Evidence Based Practice (EBP) and Evidence Informed Practice (EIP) crept into the medical vernacular only in the last ten years and these terms are now becoming more familiar to mental health professionals and educators. Why so and what do the terms actually mean? To answer, I’ll use a medical example and then take a look at the implications for school based mental health.
If you took your young child to the family doctor some years ago because of an earache, chances are following a peek into the ear revealing some redness, your doctor prescribed an antibiotic. Not so long ago a systematic review of the use of antibiotics for otitis media was published. It was found that most cases of otitis media will get better in a few days, regardless of whether antibiotics are used and antibiotics do not significantly speed up the process. This information was not available recently until many studies were systematically analyzed. These studies came not from just one expert source but from many researchers from around the world, using controlled trials where a patient was randomly assigned to treatment or no-treatment (placebo). Some of the results were conflicting but taking them all into consideration, some general conclusions were drawn. This type of evidence base from multiple sources is generally considered to be the most valid and reliable, much more so than anecdotal reports or single experiments with only one type of patient. Today, physicians are expected to be familiar with up-to-date research findings and use this knowledge in their clinical practice. Furthermore many “usual” practices, have been found to be clinically ineffective and in some cases, harmful.
In school based mental health, we are no less desirous of doing what works and avoiding doing things that are harmful. If we don’t pay heed to the evidence base, our intuitions might lead us astray. A good example is with respect to how we package the “don’t do drugs” message in schools. Having an assembly to “warn” students about the danger of drug use doesn’t work but some approaches do work. The Rand Corporation researched the Project ALERT program in 50 states in the U.S. with thousands of students and found that it is effective in curbing substance abuse. There are a number of databases of evidence-based practices, the best known is probably that of the U.S. Substance Abuse and Mental Health Services Administration (SAMHSA).
There is a subtle difference between an EBP and an EIP. An EBP is an intervention which, from research, is known to work with the problem and population to which it is addressed; whereas an EIP is the inclusion of sound evidence into approaches that take into account both professional judgment and experience. In school based mental health, it is necessary to ensure that any approaches are a good fit for the school context, are acceptable to educators and are workable in a classroom setting. In our work we are talking about three different approaches. The first is a manualized approach (following a specific program exactly); the second is a modularized approach (distilling the “active ingredients” into replicable actions, e.g. ensuring that graduated exposure is a component when dealing with anxiety) and the third is an embedded approach (i.e.: weaving the intervention naturally into the daily routines and everyday occurrences). An example of an embedded approach is to coach teachers to use collaborative problem solving as opposed to resorting a disciplinary measure for a challenging student.
There is a subtle difference between an EBP and an EIP. An EBP is an intervention which, from research, is known to work with the problem and population to which it is addressed; whereas an EIP is the inclusion of sound evidence into approaches that take into account both professional judgment and experience.
This is all still in its infancy. There are attempts to categorize interventions as: “Proven”, “Probably Effective”, “Ineffective” and “Probably harmful”. There are only a few in the top category. Furthermore, there is more to it than just knowing what works. Along with the rise of EBPs and EIPs is the growth of “implementation science”, which is the “how to” of putting scientific knowledge into practice. There is still a huge gap here.
To return to medicine, not all practices introduced today are clearly evidence-based. Just this month, a policy has just been introduced in Canada to shift the responsibility for prescribing medical marijuana to physicians from governmental control. Apparently, the effectiveness of medical marijuana in controlling pain in chronic illnesses relies solely on anecdotal accounts rather than any randomized trials or systematic reviews. The news reports indicate that doctors don’t have any guidelines about how much to prescribe and what kind of patients it is likely to work for. This seems to be a case where politics has trumped science. Go figure!
This blog post is part of CEA’s focus on student mental health, which is also connected to Education Canada Magazine’s student mental health theme issue and a Facts on Education fact sheet on what the research says about effective approaches to improving students’ mental well-being. Please contact info@cea-ace.ca if you would like to contribute a blog post to this series.
-
What is Child and Youth Mental Health?
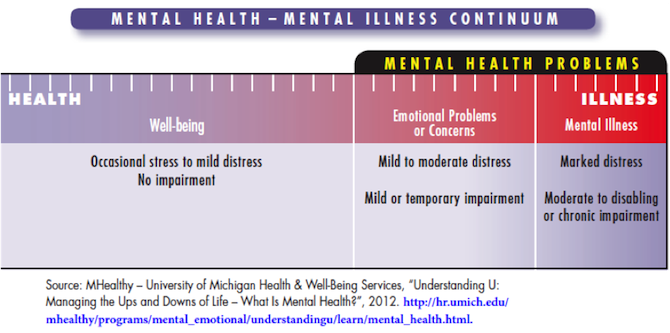
Comments Off on What is Child and Youth Mental Health?Mental Health is defined as a state of well-being in which every individual realizes his or her own potential, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to her or his community.1
Mental health problems:
- Are emotional, behavioural and brain-related difficulties that may have a negative impact on a student’s well-being;
- Interfere with the student’s functioning at school, at home, in the community, and in social settings;
- Affect the student’s development, school attendance, academic achievement, and relationships with family and friends.
A mental health problem that is severe, persistent, and causes impairment in daily life is called a mental health disorder or mental illness. It is helpful to think of mental health as occurring along a continuum.
How Common are Child and Youth Mental Health Problems?
Most estimates place the rate of mental health problems at about 18-23% of the student population. An easy way to remember how many students are affected by significant emotional difficulties is the “one in five” statistic. This means that in any given classroom of 25-30 students, there may be 5 to 7 students who struggle with behaviour and emotions to a degree that will interfere with their academic performance.
What do Mental Health Problems Look Like?
Mental health problems vary greatly in how they look. A useful way of thinking about them is to divide symptoms into two broad areas:
- externalizing problems, or behaviours like aggression, impulsivity, and non-compliance, and;
- internalizing problems, or emotional states like sadness and anxiety and behaviours like social withdrawal.
Although organizing the clusters of symptoms is useful, in real life mental health problems do not fall neatly into specific categories. Often symptoms that are associated with one disorder are also symptoms of other disorders, and, to complicate things further, disorders tend to travel together. This is called co-morbidity. Approximately 45% of children and youth with one mental health disorder are likely to have another area of difficulty as well (e.g., depression AND anxiety, ADHD AND oppositional defiant disorder).
Given how complex mental disorders are, in Ontario the only professionals who are qualified to diagnose mental health problems are physicians (including psychiatrists) and psychologists. School boards may have mental health professionals on staff who can diagnose, but many communities require a referral to children and youth mental health services.
What Mental Health Problems Are Most Likely Seen at School?
Some child and youth mental health problems are more common than others. Specifically, difficulties with anxiety, behaviour, and mood are most prevalent amongst Canadian children. Within the school context, teachers often notice emotional and behavioural difficulties associated with learning.
Within the school context, teachers are able to observe students consistently over an extended period of time. As well, they ‘see’ students in the context of other students. As such, teachers are in a unique position to notice emotional and behavioural difficulties associated with learning, and to notice when there are changes in a student’s behaviours.
Following is a list of specific student behaviours which teachers may notice and which might indicate the presence of mental health difficulties:
- social isolation
- inattention
- weak social skills
- strong emotional reactivity
- aggression
- hyperactivity /impulsivity
- poor frustration tolerance
- changes in behaviour or mood
Other general signs that a student may be struggling are when the student’s emotions and behaviour are not age appropriate, the behaviour is dramatically different from that of the student’s peers, and the duration of the behaviour appears to be excessive.
Because some mental health difficulties occur at different times in a student’s development, some types of problems are more commonly seen in primary, junior and intermediate settings, while others are most prevalent within secondary schools. Untreated problems can become more pronounced over time, and, as a result, secondary school educators are more likely to observe more serious mental health difficulties amongst students than elementary school educators. Secondary school personnel in particular, should be alert to the potential role of addictions in student emotions and behaviour at school.
Adapted from: Leading Mentally Healthy Schools: A Resource for School Administrators (School Mental Health – ASSIST, 2013) and Supporting Minds: An Educator’s Guide to Promoting Students’ Mental Health and Well-Being (Ontario Ministry of Education, 2013)
Notes
1 World Health Organization http://www.who.int/features/factfiles/mental_health/en
-
Creating More Mentally Healthy Schools
Comments Off on Creating More Mentally Healthy SchoolsThere seems to be a recent shift in the way educational institutions approach mental health. It’s an exciting time for me and the program I work for, and for all educators who just want to do their job better. It is also long overdue for families and students who are living with mental health issues. Here in Ontario, where I live and have worked as a teacher, I’m seeing giant steps in the right direction at the Ministry and Board of Education level. Hopefully this shift in approaching mental health and wellness will empower administrators, teachers and support staff to create more mentally healthy schools and ultimately improve the lives of students and their families.
It should be noted that this kind of top-down systems change is not the only exciting thing happening in student mental health. Young people can be a powerful force to initiate systems change and resource creation as well. Since its foundation in 2005, the program I work for, mindyourmind, has partnered with youth and young adults to co-create mostly web-based tools and resources around the topic of mental health. These resources are accessed by people in 195 countries, through millions of online interactions via www.mindyourmind.ca and mindyourmind’s other web platforms and social media accounts.
Hopefully this shift in approaching mental health and wellness will empower administrators, teachers and support staff to create more mentally healthy schools and ultimately improve the lives of students and their families.
As mindyourmind’s program progressed over the years, we realized that our site had become a kind of public utility – teachers and other youth-serving professionals were using our tools with their students and clients to facilitate and engage in discussions about mental health. As teachers continue to see students in need, and mental health is becomes a focus for more and more school boards across Canada, we have seen an increase in requests for resources and presentations. This may be indicative of the fact that educators want to address the topic of mental health, but may not feel like they have the time or the expertise to do so effectively.
In 2008, the Thames Valley District School Board (TVDSB) in Southwestern Ontario approached mindyourmind to develop resources for Grade 11 Physical Health Education, and Grade 9/10 Guidance and Learning Strategies. Through this collaboration, the outlines of the “Minding Your Mind” lessons were created. The lessons are digital modules which are housed online. They feature mindyourmind videos, games and interactives, are designed to meet Ministry expectations and the unique needs of the TVDSB’s populations. A teacher’s guide is included in the lessons, which offers class discussion primers and activity extension suggestions. The lessons can be self-directed by the student in a computer lab, each student clicking through and completing at their own pace, or be taught through a more facilitated approach by the teachers.
The lessons were later evaluated as part of The Mental Health Commission of Canada’s Opening Minds study, measuring the impact of different types of programs and their effect on stigma reduction. The changes in stigma and the increased social tolerance in student responses as a result of the Minding Your Mind lessons showed that this digital lesson approach was effective.
It was so encouraging to see actual research support what mindyourmind already felt about the work that we are doing: Creating resources with young people works. Our tools do a great job of presenting information effectively and in a way that is relevant to youth, and can help teachers address what can be a tricky topic for some in a positive way.
How do we insert mental health info into a Civics class, or a Writer’s Craft class, without disrupting what the teacher needs to get done in an already saturated course workload?
My role here at mindyourmind is to develop more resources that will help teachers bring conversations about mental health into their classrooms, even in subjects that wouldn’t normally directly address mental health. I’ve heard some compare this task to “hiding the vegetables”. How do we insert mental health info into a Civics class, or a Writer’s Craft class, without disrupting what the teacher needs to get done in an already saturated course workload? We have a few projects on the go, including a resource for dance educators, which is being piloted this spring. It’s exciting work!
If you are a teacher, how do you support conversations about mental health in your classroom? How might you address mental health while teaching a course that doesn’t explicitly ask you to in the curriculum?
This blog post is part of CEA’s focus on student mental health, which is also connected to Education Canada Magazine’s student mental health theme issue and a Facts on Education fact sheet on what the research says about effective approaches to improving students’ mental well-being. Please contact info@cea-ace.ca if you would like to contribute a blog post to this series.
-
How to Stop Hurting Yourself
Comments Off on How to Stop Hurting YourselfThis content has been re-posted from Erin Schulthies Blog at: http://daisiesandbruises.com/2014/03/03/how-to-stop-hurting-yourself
Most Google searches leading to this blog involve the words, “hurt myself.” So many people are looking for help in stopping self-harm, stopping cutting, bruising or any other kind of self-hurting.
Self-harm is something I know a lot about. I could write hundreds of posts on the topic (and I probably will), but for now, I have two pieces of advice that are my secrets to stopping self-harm.
1) LET YOURSELF FEEL
No feeling is wrong. Absolutely every single emotion you have is legitimate and allowed. Read that sentence again: Absolutely every emotion you have is legitimate and allowed. Sometimes we don’t understand our feelings, where they’re coming from or why, but that shouldn’t stand in our way of permitting ourselves to feel exactly how we’re feeling. Let yourself feel and identify the feeling if you can. Say to yourself, “I feel _______.”
2) EXPRESS YOUR FEELINGS
You can’t skip this step. This is the answer to stopping self-harm: Allow yourself to express your emotions in a way that doesn’t involve hurting yourself.
Here are some ideas:
Talk to someone, cry, scream, whimper, holler, write, play music, run, dance, or tear up pieces of paper. Go out into a field and throw rocks at the sky. Don’t just punch your pillow, pummel it. Run faster than you’ve ever run before. Use the energy created by your feelings and do something with it.
A lot of the feelings I first expressed through cutting were related to my memories of violence. I felt hurt and damaged and I wanted to damage something to communicate my pain. So I damaged myself.
But, do you know what? You can damage things other than yourself. Never damage another living thing and try not to damage property that isn’t yours, but if you want to destroy something, IT DOESN’T HAVE TO BE YOU.
Emotions don’t always feel nice and pretty and socially acceptable. I used to cut because I didn’t want to be nice or pretty or socially acceptable. I wanted the whole fucking world to know just how terrible I felt.
Hurting myself didn’t help me feel better. It hurt me! And there is enough hurt without me hurting myself extra. You can’t get better if you hurt yourself.
Writing and making art works a MILLION times better for me than cutting ever did. Remember my drawing from my last hospital stay? It showed black swirls of monstrous arms attacking me. Drawing that helped me feel SO MUCH BETTER. And I showed it to people, I said, “THIS is how bad I’m feeling.” No, it’s not art for a museum. It’s art for me. And it worked.
Go ahead, be destructive if it doesn’t hurt anyone. Let yourself feel and then express those feelings in a healthy way. Never pretend to feel something that you don’t feel. Be honest about what’s in your heart and it will heal you, I promise.
This blog post is part of CEA’s focus on student mental health, which is also connected to Education Canada Magazine’s student mental health theme issue and a Facts on Education fact sheet on what the research says about effective approaches to improving students’ mental well-being. Please contact info@cea-ace.ca if you would like to contribute a blog post to this series.
-
What should you do if you suspect mental illness in a student?
Comments Off on What should you do if you suspect mental illness in a student?One in five youth under the age of 18 has a diagnosable mental disorder. So in a classroom of 25 children, you can expect five to be struggling with significant emotional problems. How can you recognize the signs? What should you do if you see them?
Kids develop along different dimensions: physical, social, familial, emotional, cultural, psychological. And there’s a continuum between “normal” and “abnormal”. Most mental illnesses represent an interaction between nature and nurture, and result in a failure of that child to be able to meet their “developmental tasks” (age-appropriate expectations) in the dimensions just mentioned.
So, recent changes in behaviour that are unusually intense, frequent, and persistent for that child, should catch your attention. The definition of mental illness is basically subjective distress (“I don’t feel happy”) plus functional impairment (“I just can’t do what I used to do, or what my parents/friends expect me to do.”). A combination of these features is highly suggestive that the student is in trouble.
Practically speaking, this can look like:
- changes in sleep, appetite, or energy level;
- social withdrawal or aggression;
- new conflict with parents;
- sadness, worry, or irritability and lack of self-esteem.
In the classroom, concentration, memory, organization, and participation can all be affected, with the net result being assignments not handed in and marks going down.
Risk factors for mental illness include:
- recent physical illness in the student or a family member;
- a family history of mental illness;
- insult to the student’s brain (e.g. concussion);
- lack of stable attachment figures (e.g. high conflict divorce, death of a loved one, or frequent moves);
- single parenthood and poverty; neglect, abuse, or being the victim of bullying;
- standing out as “different” for any reason (height, weight, intellectual capacity);
- and difficult temperament (poor self-regulation, prone to hyper-sensitivity and hyper-reactivity).
What should you do if you suspect mental illness in a student?
- Get help – don’t shoulder the burden alone!
- Go slowly – talk to the student directly, and enquire about how things are going for him/her. Then voice your concerns, describing them in a neutral, non-judgmental, and behaviourally verifiable way (“I’ve noticed that lately you’ve stopped playing with your friends at recess, you’re more quiet than usual, and you’re not at the soccer games as much as before. Is anything going on that you’d like to talk about?”)
- Involve the parents – no student is an island, and often comparing your notes with the parents in extremely informative. If the parents share your concerns, suggest that they contact their family doctor or pediatrician to make sure there isn’t a physical illness. Once that is ruled out, together you can talk about whether a referral to a mental health specialist is warranted.
The good news in all this is that when mental illness is identified and treated early, the prognosis is excellent. Seventy-five per cent of mental illnesses begin before the age of 20, but because the brains and environments of children are still changeable (“plastic”), the vast majority of youth can overcome their struggles and resume their course of normal development, flourishing, and reaching their natural potential.
PS: A great resource for parents and teachers is The ABC’s of Mental Health, a free, on-line resource developed by the Hincks-Dellcrest Centre for Children and Families.
This blog post is part of CEA’s focus on student mental health, which is also connected to Education Canada Magazine’s student mental health theme issue and a Facts on Education fact sheet on what the research says about effective approaches to improving students’ mental well-being. Please contact info@cea-ace.ca if you would like to contribute a blog post to this series.
-
Taking mental health to school
Comments Off on Taking mental health to schoolAs I was editing the articles in this issue, an online fundraising campaign was launched in my community to raise money for a young woman who desperately needed intensive residential treatment for her eating disorder – a program not funded by our provincial health plan. She wrote eloquently about her inability to fight the disease on her own, her fear of dying, and the hopelessness that long wait lists engender in a young person who needs help now.
It’s a heartbreaking story that illustrates perfectly the “fractured system” that Kate Tilleczek and Katherine Lezeu describe in “Journeys in Youth Mental Health” (p. 12) – and yet it also gives me hope. It gives me hope because not so long ago, we would not have even heard this girl’s story, or had a chance to help (when I last checked, $36,000 had been donated). This girl and her family would have suffered in silence: the taboo around disclosing mental illness was too strong.
The uneasy impression I had when my sons were in high school – that more kids than ever before are struggling with mental health problems – is confirmed in this issue. But beyond the worrying statistics, something good is happening. Young adults I know (or know of, through my kids) are talking about their struggles. They are also blogging, advocating, and starting virtual support groups. When yet another gay teen commits suicide, or a mentally ill man “armed” with a screwdriver is shot by police, they are not just saddened – they are outraged. I know not all young people have this level of awareness, but I do believe they are leading a sea change in our public understanding of mental health.
How can we, as educators, help? Our students bring their troubles to school with them, and too often face troubles at school. School leaders tell us they are searching for ways to support the many students struggling with mental health issues, yet it seems an overwhelming challenge. In this issue, we explore how we can “take mental health to school,” and share some initiatives that have been successful at reducing stigma and building knowledge. Schools are not treatment facilities, and they can’t make up for the failings of a fractured system – but they can be an important part of the solution.
P.S. Check out our web exclusive article, “Minding Your Mind,” to learn about a school mental health program developed in partnership with the non-profit youth mental health initiative mindyourmind: www.cea-ace.ca/educationcanada
This blog post is part of CEA’s focus on student mental health, which is also connected to Education Canada Magazine’s student mental health theme issue and a Facts on Education fact sheet on what the research says about effective approaches to improving students’ mental well-being. Please contact info@cea-ace.ca if you would like to contribute a blog post to this series.
-
Dr. Kate Tilleczek: 2013 CEA Whitworth Award Winner
Comments Off on Dr. Kate Tilleczek: 2013 CEA Whitworth Award Winner2013 CEA Whitworth Award for Career Research in Education for Her Sustained Focus on Students on the Margins
http://vimeo.com/90975544
-
Taking mental health to school
Comments Off on Taking mental health to schoolAs I was editing the articles in this issue, an online fundraising campaign was launched in my community to raise money for a young woman who desperately needed intensive residential treatment for her eating disorder – a program not funded by our provincial health plan. She wrote eloquently about her inability to fight the disease on her own, her fear of dying, and the hopelessness that long wait lists engender in a young person who needs help now.
It’s a heartbreaking story that illustrates perfectly the “fractured system” that Kate Tilleczek and Katherine Lezeu describe in “Journeys in Youth Mental Health” (p. 12) – and yet it also gives me hope. It gives me hope because not so long ago, we would not have even heard this girl’s story, or had a chance to help (when I last checked, $36,000 had been donated). This girl and her family would have suffered in silence: the taboo around disclosing mental illness was too strong.
The uneasy impression I had when my sons were in high school – that more kids than ever before are struggling with mental health problems – is confirmed in this issue. But beyond the worrying statistics, something good is happening. Young adults I know (or know of, through my kids) are talking about their struggles. They are also blogging, advocating, and starting virtual support groups. When yet another gay teen commits suicide, or a mentally ill man “armed” with a screwdriver is shot by police, they are not just saddened – they are outraged. I know not all young people have this level of awareness, but I do believe they are leading a sea change in our public understanding of mental health.
How can we, as educators, help? Our students bring their troubles to school with them, and too often face troubles at school. School leaders tell us they are searching for ways to support the many students struggling with mental health issues, yet it seems an overwhelming challenge. In this issue, we explore how we can “take mental health to school,” and share some initiatives that have been successful at reducing stigma and building knowledge. Schools are not treatment facilities, and they can’t make up for the failings of a fractured system – but they can be an important part of the solution.
P.S. Check out our web exclusive article, “Minding Your Mind,” to learn about a school mental health program developed in partnership with the non-profit youth mental health initiative mindyourmind: www.cea-ace.ca/educationcanada
Write to us!
Send your letters or article proposals to editor@cea-ace.ca, or post your comments on the online version of Education Canada at: www.cea-ace.ca/educationcanada.
Photo: Dave Donald
First published in Education Canada, March 2014
-
13-Point Bullying Prevention Plan
Comments Off on 13-Point Bullying Prevention PlanHow can a school combat bullying? This article outlines a 13-Point Bullying Prevention Plan that can be led by the principal of any school to both reduce the amount of bullying and provide a safety net for those affected by it. While there is really “nothing new” regarding each of the 13 points, my experience over 14 years as a school superintendent in charge of safe schools in a southwestern Ontario school district is that when a school adheres to all of them, there will be a reduction in bullying. These 13 elements in bullying prevention do not carry a financial requirement for schools and rely on effective principal leadership. What the 13-Point Bullying Prevention Plan is not about, however, is a “quick fix.” Successful bullying prevention in schools requires the united efforts of the staff and school community.
1. Involve the entire school community
It is very important that staff, starting with the principal and including all teaching staff and anyone else who works in the school – educational assistants, bus drivers, support personnel, and parent volunteers – be actively aware of bullying and able to address it. The school community must be on board with bullying prevention. Only through the concerted efforts of the school staff, in conjunction with the school community, can bullying be acted on both at school and at home. Start by providing bullying prevention information to the school community at the start of each school year, as well as outlining the consequences for bullying behaviour.
As well, some class time should be devoted on an ongoing basis to discussing bullying and peer relationships with students. Bullying prevention themes and messages can be incorporated into daily activities and can be displayed in hallways and classrooms. It is critical that the bully prevention focus is not simply given “lip service” by staff. It must genuinely be a priority within the school and must rank as a topic of importance alongside literacy, numeracy, and secondary graduation rates.
2. Establish a bullying prevention committee
The principal, as leader of the school, should establish and lead a bullying prevention committee, with membership comprising representative teachers from different divisions or departments, non-teaching staff, and several parents from the school community. It is the responsibility of this committee to direct the bullying prevention initiative of the school. Since the principal has the legal authority to mete out discipline to students found guilty of bullying, it is appropriate that he or she be the leader of the committee. The committee cannot be allowed to stagnate; membership needs to be changed periodically but the principal remains the key driving force as, ultimately, the effectiveness of any bullying prevention plans rests with him or her.
3. Create a caring school climate
For any bullying prevention program to be truly effective, the atmosphere of the school must be warm and inviting. What does that mean? A warm and inviting school is one in which the staff take pride in their school and there are obvious signs of positive learning. Parent and visitors to the school are made to feel welcome by all staff; student work and awards are prominently displayed; staff greet students in the hallways; and there is a feeling of belonging within the building by all who work and study there. Both staff and students work in an atmosphere of mutual respect. Student discipline is fair, appropriate to the circumstances and judiciously applied. Teachers take a personal interest in all of their students.
A school environment that is supportive, friendly and caring is not conducive to bullying; moreover, it is far easier for victims of bullying to obtain help and assistance in such a setting. Bullies can thrive in schools that do not provide an inclusive, caring, and accepting environment.
4. Implement a school climate survey
How does a school know where to start when addressing bullying? The answer begins with a school climate survey. Students, parents, and staff are surveyed about their perceptions of the school atmosphere, and specific questions about bullying that need to be posed, including how much bullying occurs and where it frequently takes place. Repeat the survey at least every two years to monitor any changes within the school community over time. This information can then be used by the bullying prevention committee to map out next steps. Each school is different in staff composition, student demographics, and physical plan; so, results garnered from the surveys will help pinpoint issues related to bullying that are unique to each building.
5. Identify school “hot spots”
Each school has certain locations where bullying is far more prevalent. Such “hot spots” necessitate increased adult supervision. At elementary schools, hot spots for bullying usually include the playground and on the buses to and from school. Change rooms for physical education and the cafeteria are places where bullying occurs in both elementary and secondary schools because there is minimal or no direct supervision. Class change times, when students are moving between classes in the hallways, are prime bullying opportunities in middle and secondary schools. All of these potential hot spots should be identified and the school bullying prevention committee must create a plan to provide more adult supervision in these areas, both as a deterrent and so that bullying can be quickly identified and acted upon.
6. Ensure teachers know how to deal with bullying
All staff should feel capable of effectively intervening in a bullying situation. When teachers observe bullying, they need to take direct and swift action to end it on the spot. Teachers should be able to support victims and help them to “save face” and calm down. Intervention by teachers into instances of bullying should be routinely and consistently carried out. All staff require some training on what bullying “looks like” and how important it is to nip the bullying quickly before it becomes more entrenched. Up-to-date literature regarding bullying can be disseminated to staff by the school’s bullying prevention committee. A good resource for both teachers and administrators can be found at www.prevnet.ca.
7. Teach students bullying prevention strategies
Inevitably, some students are going to be victimized. Those who do not have a cluster of friends to support them will be vulnerable. Students who have minimal friendships and who are non-assertive are at greater risk of being bullied. It is important that schools teach tactics to help students avoid becoming the victims of bullying.
Students also need to be made clearly aware of the potential risks that abound with current Internet access. Students should know that if they receive unwanted electronic communication they can IGNORE, BLOCK, and REPORT it.8. Establish clear, consistent consequences for bullying behaviour
Schools must have clear and explicit expectations that bullying behaviour will not be tolerated. School rules/codes of conduct must identify that bullying of all kinds will be dealt with using progressive discipline. There must be teeth to the rules – appropriate consequences, from detention to suspension to possible expulsion for serious incidents, are part of the principal’s arsenal so that the school community fully understands that individual student safety must be upheld.
Bullies also require support and counselling to help them change their behaviour and acquire empathy for their victims. The principal needs to involve the bully and his or her parents. Efforts to counsel the bully must be coupled with clear disciplinary action that lets the school community know, in no uncertain terms, that bullying is not tolerated.
9. Don’t turn a blind eye to cyberbullying
Cyberbullying is definitely here to stay. The rapidly changing and more sophisticated means that students now have to communicate with (and about) one another is a complex issue that must be dealt with by school administrators. Gone are the days when principals could reason that if it “didn’t happen at school” or “it didn’t happen during school hours” they need not deal with cyberbullying. On the contrary, when students target and bully other students through various electronic means, principals have an obligation to investigate, and when necessary, impose disciplinary consequences.
A constant bombardment of cyberbullying can have a devastating impact on young people. When a student of any age is targeted through the use of e-mail, texting, sexting, Facebook, Twitter, or other means, the victim is at risk of emotional traumatization. This is not conducive to learning and must be brought to the attention of the school administrator. When it is, principals must investigate just as they would any other alleged misbehaviour involving students.
A tremendous resource for both teachers and school administrators can be found at www.cyberbullying.us. This site is managed by two American experts in cyberbullying, Dr. Justin Patchin and Dr. Sameer Hinduja, who are co-directors of the Cyberbullying Research Center in the U.S.
10. Establish a school bullying tracking system
A means of tracking bullying incidents at schools – whether it is the tried-and-true binder containing a list of bullying incidents or an electronic database – is essential. The reason is quite simple: aggressors bully repeatedly. By having a constantly updated file listing all such infractions, principals have names, dates, types of incidents and consequences at their fingertips. As a result, a profile of who is victimized and who is doing the bullying can be accurately identified. Progressive discipline can be used on offenders while support can be provided to the victims. The most important benefit of such a tracking system, however, is the impact that it has on the student body. Students soon realize that bullying is being closely monitored and that there are clear, negative consequences in store for all who bully. Bullies are more closely watched by school staff because of their “track record.”
Gone are the days when principals could reason that if it “didn’t happen at school” or it “didn’t happen during school hours” they need not deal with cyberbullying.
11. Establish a confidential reporting system
A confidential reporting system does not need to be an elaborate set-up that requires much time and effort. Some schools employ a “talking locker” where students can leave anonymous notes identifying bullies and/or victims. Some secondary schools have employed electronic communication between students and school administrators via a link from the school webpage. Whatever method is used, the critical issue is that there is a vehicle available for students to be able to let the school authorities know, in a confidential way, of victimization that is taking place.
Just having the principal walking the hallways and grounds of the school is a useful strategy. When a principal is consistently present in the hallways and classrooms at class change, recess and lunch time, he or she gains valuable insights regarding student behaviour. By careful observation, an astute principal can sense when a student has been marginalized and potentially targeted. Potential targets of bullying can be identified and referred to the school’s bullying prevention committee.
12. School staff must provide support for victims of bullying
This is a critical requirement for an effective school response to any form of bullying. Victims of bullying need support to clarify the truth that what they have been subjected to was wrong and must not continue. Whether speaking to a classroom teacher, an educational assistant, a social worker, a child and youth worker, or a guidance counsellor, victims need to be able to sit with someone and express their feelings about being bullied and receive individual support and counselling.
13. Bring new staff members into the program
One of the many challenges that principals face is constant and ongoing staff changes each year. Principals need to ensure that all incoming staff members are immersed in bullying prevention policies and procedures. New staff members who may not understand the potential damaging impact of bullying need to receive this information upon their arrival. Buddying up teachers new to a school with experienced staff who can mentor them on how the school “deals” with bullying is a way to quickly help the new faculty recognize and understand the importance of student safety and the prevention of victimization. As obvious as it seems, students should be able to count on school staff for protection from bullying and it is important that new staff recognize what to look for and how to respond when bullying occurs.
The 13-point Bullying Prevention Plan has no costs associated with its implementation and will have a significant impact on reducing school bullying. I encourage you to try it at your school.
Photo: iStock
First published in Education Canada, March 2014
EN BREF – Comment une école peut-elle combattre l’intimidation? Cet article énonce un programme en 13 points de prévention de l’intimidation que peut mener la direction de n’importe quelle école à la fois pour réduire la fréquence de l’intimidation et pour fournir un filet de sécurité aux personnes touchées. Bien que ces 13 points ne comportent rien de vraiment nouveau, l’intimidation diminue lorsqu’une école les instaure tous, d’après l’expérience de plus de 14 ans de l’auteur à titre de surintendant responsable de la sécurité dans les écoles d’un conseil scolaire du sud-ouest de l’Ontario. Ces 13 éléments de prévention de l’intimidation n’imposent pas de charge financière aux écoles et s’appuient sur un leadership efficace de la direction d’école et sur les efforts conjoints du personnel et de la communauté scolaire.
-
School Mental Health Literacy
Comments Off on School Mental Health LiteracyThe increasing global awareness of the need to address youth mental health in the school setting is now spreading across Canada. Numerous initiatives at the school, school board and policy (provincial and territorial) levels have begun to develop. Evergreen, the national child and youth mental health framework created under the direction of the Mental Health Commission of Canada,1 identified the importance of developing school mental health initiatives as part of a comprehensive approach to addressing the complex mental health needs of young people. The recent national report by the School-Based Mental Health and Substance Abuse Consortium2 and national child and youth mental health policy development documents, such as the Canadian Institutes of Health Research white paper on access and wait times in child and youth mental health,3 have further highlighted the importance of this issue nationwide.
Many approaches to addressing the complexities of school mental health have been applied and studied. While the results have been mixed and hopes for universal interventions leading to significant and substantial positive mental health results have not yet been achieved,4 much has been learned and these lessons can help us here in Canada bring a more thoughtful and informed approach to addressing school mental health. Two important lessons have to do with:
- the need for research-based interventions that achieve sustainable positive results by building on the existing ecological strengths of schools; and
- the importance of creating integration across the many separate systems traditionally involved in providing human services to young people (education, health, child welfare, etc.).
Such approaches can avoid the high-cost and often less-than-effective “program in a box” applications so commonly being applied to address mental health in school settings and can be designed to meet specific mental health needs of young people within the context of local realities.
Foundational to all school mental health domains is the need to effectively address the mental health literacy of students, educators and administrators alike. Like any form of literacy, mental health literacy is a foundational component upon which additional structures – such as mental health promotion, validated and effective prevention, enhanced access to the most appropriate mental health care, etc. – can be built.
Early approaches to addressing mental health literacy were often one-dimensional, focusing mostly on addressing one mental disorder, such as depression. They were not contextualized to the school setting, not designed to fit into students’ usual class/course-based educational experiences, and not related to existing school ecologies. Moreover, they were often applied in isolation from existing health and human services organizations that needed to be included to meet student’s mental health care needs. As a result, according to a recent systematic review of school-based mental health literacy interventions,5 the positive results of these early applications were difficult to determine. A more recent Canadian approach has been informed by the need to widen the concept of mental health literacy and to create interventions that are student-, teacher- and administration-friendly, easily integrated into the school curriculum, sustainable and inexpensive to apply. Further, this approach facilitates horizontal integration across existing human services systems and builds upon the professional capabilities of teachers, as described in the School-Based Integrated Pathway to Care Model for Canadian Secondary Schools.6
Mental health literacy in the junior high and high school setting can be defined as having four unique but integrated components:
- understanding how to foster and maintain good mental health;
- understanding mental disorders and their treatments;
- decreasing stigma; and
- seeking help effectively.
In order to help address mental health literacy in the Canadian school setting, the Canadian Mental Health Association, in collaboration with Dr. Kutcher, created and field tested the Mental Health & High School Curriculum Guide (hereafter the Guide), a resource for teachers designed for classroom use primarily in Grades 9 and 10. This target point was chosen because of the data that demonstrates a rapid increase in the onset of mental disorders beginning around the onset of puberty and lasting until about age 25.7
Written in collaboration between educators and mental health professionals, the Guide underwent extensive field tests and multiple modifications based on those tests. It addresses mental health literacy in the classroom through six teacher-ready, online-available modules (http://teenmentalhealth.org/curriculum) covering:
- the stigma of mental illness;
- understanding mental health and mental illness;
- information on specific mental illnesses;
- first-person experiences of mental illness;
- seeking help and finding support;
- the importance of positive mental health.
Teacher self-study and face-to-face training programs to support the classroom application of the Guide were created, and extensively evaluated with highly positive outcomes.[8] Both the teacher training programs and classroom application were implemented in the Province of Nova Scotia. There, the Guide was applied by teachers trained in its use by school board-based training teams and used to meet the provincial curriculum standards in the Healthy Living course taken by all Grade 9 students. This has been followed by widespread school- and board-level applications in various jurisdictions across Canada.
Evaluation results for seven English school boards in N.S.9 demonstrate that the teacher training program on the classroom use of this resource significantly and substantially increased teachers’ knowledge about mental health (Figure 1). In addition, the training program significantly and substantially decreased participants’ mental health related stigma (Figure 2). It is noticeable that participants’ attitudes towards mental illness were highly positive before the training, yet even so, their attitudes were substantially enhanced after the training.
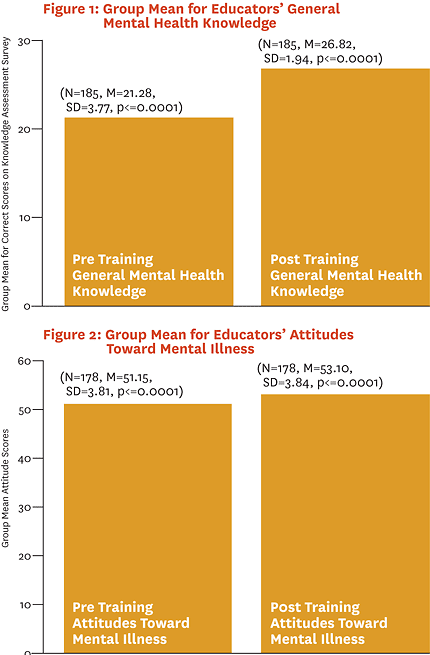
In other words, the data demonstrate that simply providing training to teachers on how to use the Mental Health Curriculum Guide resource and helping them integrate this resource into their existing professional competencies has significant and substantial positive impacts on their own mental health literacy. This occurs without creating and delivering a stand-alone teachers’ mental health program or exposing teachers to non-contextualized, expensive and less impactful universal approaches. Participants further provided overwhelmingly positive comments on this training program. Some examples from teachers include:
Thank you for a curriculum that includes mental health! This guide and in-service is are great resources.
I truly appreciate all of the resources. I feel I wasn’t simply told to be better, but shown how to teach mental health better. I wish all outcomes were addressed in this manner. Thank you. Very interesting information and useful resources.
In addition, two large independent research studies conducted in Ontario have demonstrated similar significant and substantial impacts of the classroom curriculum approach using the Mental Health Curriculum Guide on students. A study using a case-controlled cohort design conducted in a number of school boards demonstrated that students exposed to the curriculum in the classroom substantively improved their mental health literacy, showing increased knowledge and decreased stigma from pre-test to post-test.[10] These positive impacts in knowledge and attitudes were maintained over a two-month follow-up. Further, a randomized, controlled trial in 25 Ottawa schools demonstrated similar outcomes, as well as significant improvement in student-reported help-seeking efficacy.11 Qualitative feedback from teachers was positive and identified ease in classroom application and no demonstrated negative outcomes. Quotes from teachers and students include:
Before this mental health unit, I thought that people with a mental illness couldn’t have a normal life and couldn’t have any friends. I also thought that people with a mental illness could get better if they wanted to but I know that they can’t do it by themselves and they need help from family, friends, counselors etc. – an Ontario student
Thank you for a very meaningful and informative session. Very valuable and important information for all teachers. – an Ontario teacher
Similar studies in other locations, including globally in countries as different as Malawi and Brazil, have been implemented and are awaiting completion.
How to Access the Mental Health Curriculum Guide
- The Mental Health Curriculum Guide resource is now available online: http://teenmentalhealth.org/curriculum
- The Guide includes lesson plans, classroom resources (e.g. first-person and animated videos), teaching resources (e.g. handouts and web-based directions for information retrieval), student evaluations, etc. Further enhancement of this material for use by teachers is underway with the development of an enhanced pre-screened and validated resource kit that will be posted soon.
- Information about training programs for use of the Mental Health Curriculum Guide is also available through: www.teenmentalhealth.org
- For more information, email inquiries to: info@teenmentalhealth.org
Overall, this approach to addressing mental health literacy as the foundation for mental health promotion, prevention and care in teachers and students is based on utilizing the existing ecological strengths of schools and the professional competencies of teachers instead of parachuting costly stand-alone programs into schools. It provides a relatively simple, economical and effective method to improve knowledge, decrease stigma and enhance help-seeking efficacy in both teachers and students. This approach mirrors the method by which teachers usually learn and prepare for their teaching, and by integrating student learning about mental health into existing curriculum, it avoids isolating mental health from everyday school activities. The creation of school board-based training teams that can meet training needs in-house enhances the probability of sustainable integration at minimal cost. Positive results have been found in every school in Canada where the resource has been applied and evaluated, thus making it feasible for use across the diverse Canadian mosaic.
Photo: iStock
First published in Education Canada, March 2014
EN BREF – La sensibilisation mondiale croissante à l’égard de la nécessité de porter attention à la santé mentale des jeunes dans un cadre scolaire s’étend actuellement au Canada.
L’article décrit La santé mentale et l’école secondaire – Guide de formation, une ressource nationale en matière de formation en santé mentale à l’école qui a été instaurée et a fait l’objet d’études dans des écoles secondaires (9e et 10e années / 3e et 4e secondaire) partout au Canada. Il est question du contenu du guide et de ses processus d’instauration qui peuvent être contextualisés pour répondre aux besoins des élèves, quelle que soit l’école fréquentée. L’article présente également les plus récents résultats de recherche et d’évaluation de l’application du guide, lesquels font état de connaissances considérablement enrichies, d’une stigmatisation moindre et d’une efficacité accrue de la recherche d’aide chez les élèves et les éducateurs qui l’ont utilisé dans le cadre du curriculum scolaire habituel.
[1] S. Kutcher and A. McLuckie for the Child and Youth Advisory Committee, Evergreen: A child and youth mental health framework for Canada(Calgary, AB: Mental Health Commission of Canada, 2010).
[2] School-Based Mental Health and Substance Abuse Consortium (supported by the Mental Health Commission of Canada), Survey on School-Based Mental Health and Addictions Services in Canada (April 2012).
[3] The Canadian Association of Paediatric Health Centres, The National Infant, Child, and Youth Mental Health Consortium Advisory, and The Provincial Centre of Excellence for Child and Youth Mental Health at CHEO, Access and Wait Times in Child and Youth Mental Health: A background paper, for the Institute of Human Development, Child and Youth Health (Oct. 2010).www.excellenceforchildandyouth.ca/sites/default/files/policy_access_and_wait_times.pdf
[4] K. Weare and M. Nind, “Mental Health Promotion and Problem Prevention in Schools: What does the evidence say?” Health Promotion International 26, Suppl. 1 (Dec. 2011): i29-69.
[5] Y. Wei, J. Hayden, S. Kutcher, A. Zygmunt, and P. McGrath, “The Effectiveness of School Mental Health Literacy Programs to Address Knowledge, Attitudes, and Help-Seeking among Youth,” Early Intervention Psychiatry 7, no. 2 (May 2013): 109-21.
[6] Y. Wei, S. Kutcher, and M. Szumilas, “Comprehensive School Mental Health: An integrated ‘School-Based Pathway to Care’ model for Canadian secondary schools,” McGill Journal of Education 46, no. 2 (2012): 213-229.
[7] R. C. Kessler, P. Berglund, O. Demier, R. Jin, K. R. Merikangas, and E. E. Walters, “Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication,” Archives of General Psychiatry 62, no. 6 (June 2005): 593-602.
[8] S. Kutcher, Y. Wei, A. McLuckie, and L. Bullock, “Educator Mental Health Literacy: A program evaluation of the teacher training training education on the mental health & high school curriculum guide,” Advances in School Mental Health Promotion (2013); A. McLuckie, S. Kutcher, Y. Wei and C. Weaver, “Sustained Improvements in Students’ and Teachers’ Mental Health Literacy with Use of a Mental Health Curriculum in Canadian Schools,” unpublished manuscript (Sun Life Financial Chair in Adolescent Mental Health, 2013).
[9] Sun Life Financial Chair in Adolescent Mental Health, “Mental Health & High School Curriculum Guide Training Report for Nova Scotia,” (2013).http://teenmentalhealth.org/images/uploads/mental_health_curriculum_guide_training_NS_final_July_25_2013.pdf
[10] McLuckie et al., “Sustained Improvements in Students’ and Teachers’ Mental Health Literacy.”
[11] R. Milin, S. Kutcher, S. Lewis, S. Walker, and N. Ferrill, “Randomized Controlled Trial of a School-Based Mental Health Literacy Intervention for Youth: Impact on knowledge, attitudes, and help-seeking efficacy” (poster presentation at American Academy of Child and Adolescent Psychiatry 60th Annual Meeting, 2013).
-
Teen Stress in Our Schools
Comments Off on Teen Stress in Our SchoolsFor the average high school student, life is full of potential stressors. In a recent survey, our research team asked over 900 Grade 7 students what they identified as the biggest stressors in their lives. “Academic difficulties” was reported as the greatest stressor by 33.2 percent of students, followed by “conflict with parents/family” (31.4 percent), “conflict with peers” (20.7 percent), and “conflict between parents” (13.9 percent). Of particular concern is how these students are coping with their stress.[1]
-
What are effective approaches to improving students’ mental well-being?
Comments Off on What are effective approaches to improving students’ mental well-being?Youth mental health is of great concern in Canada and around the world. The Canadian Mental Health Association estimates that 10-20% of Canadian youth are affected by a mental disorder; other studies indicate even higher rates of depression, behavioural issues, and bullying in school settings. In addition to problems with attendance associated with these issues, learning is also often negatively impacted. Many researchers and practitioners believe that incorporating mental health programming into curricula is critical to addressing this issue. When the Mental Health Commission of Canada released the nation’s first national mental health strategy in 2012, child and youth mental health was identified as a priority and school-based programs were suggested as an effective tool to promote mental health.
Many programs have been implemented on a board, district, or provincial level in Canada; a recent scan published by the School-based Mental Health and Substance Abuse (SBMHSA) consortium identified over 100 programs currently in use across the country. The challenge in determining which programs are most effective lies in the lack of evidence-based research. While the body of research around school-based mental health programs is growing steadily, it is scattered, often evaluating a single program in a single setting and few programs have more than one or two evaluations. Based on this limited evidence, two programs were strongly recommended in the Social Emotional Learning (SEL) Toolkit developed by the Canadian Prevention Science Cluster (Atlantic). They are Promoting Alternative Thinking Strategies (PATHS) and Second Step. Another program, Zippy’s Friends, achieved positive results in a Quebec study.
Despite the scattered nature of program evaluation, the research that does exist indicates a common understanding on the characteristics of an effective program. School based programs should:
- be part of a comprehensive school health initiative and reach all students rather than targeting those identified as having mental health issues;
- be collaborative – with educators, students, parents, community agencies, and health providers working together;
- focus on promotion of positive mental health rather than reaction to mental illness;
- be adaptable to meet the needs and resources of the setting.
Additionally, attention must be paid to how programs are implemented in schools. Even when adapted to suit the local circumstances, programs must be delivered with fidelity to the original design. The process and outcomes must be closely monitored to ensure the desired results are achieved. Resources need to be available for training and support of program delivery personnel.
The mental well-being of children and youth is a critical issue for parents, educators, health care providers, researchers, and policy-makers. These groups need to work together not only to continue gathering evidence on programming models, but to also begin building effective or promising programs into curricula now.
CHILD AND YOUTH MENTAL HEALTH PROGRAMMING
CHILD AND YOUTH MENTAL HEALTH ORGANIZATIONS AND ONLINE RESOURCES
- School Mental Health Assist
- First Call – B.C. Child and Youth Advocacy Coalition
- Canadian Health & Youth Health Coalition
- Teen Mental Health
- Related Videos
- Centre for Addiction and Mental Health (CAMH)
- Ontario Public School Boards Association
- Canadian Prevention Science Cluster – Atlantic
- Canadian Prevention Science Cluster
- Pan-Canadian Consortium on Youth Mental Health – Positive Mental Health Toolkit
- Fast Facts about Mental Illness – Canadian Mental Health Association
- Improving Health and Wellbeing for Children and Youth in Challenging Contexts
- International Alliance for Child and Adolescent Mental Health and Schools
- OPHEA
- Partners for Mental Health
MENTAL HEALTH WEBSITES FOR YOUTH
CHILD AND YOUTH MENTAL HEALTH PROGRAM SCANS
- A Scan of Canadian Practices – School Based Mental Health and Substance Abuse Consortium
- Blueprints for Healthy Youth Development – Centre for the Study of Prevention of Violence
- What Works Clearinghouse – Institute of Educational Sciences
- CASEL Guide – Effective Social and Emotional Learning Programs
REFERENCES
Dufour, S., Denoncourt, J., & Mishara, B. L. (2011). Improving children’s adaptation: New evidence regarding the effectiveness of Zippy’s Friends, a school mental health promotion program. Advances in School Mental Health Promotion, 4(3), 18-28.
Government of Alberta. (2013). Mental health capacity building in schools initiative. Author.
Guyn Cooper Research Associates. (2013). Issue brief: Social and emotional learning in Canada. Carthy Foundation and Max Bell Foundation.
Kutcher, S. (2013). Bringing schools to mental health and bringing mental health to schools: Challenges, confusions and opportunities. MASS Journal, Spring, 12-15.
Kutcher, S., McLuckie, A., & Child for Youth Advisory Committee, Mental Health Commission of Canada. (2010). Evergreen: A child and youth mental health framework for Canada. Calgary, AB: Mental Health Commission of Canada.
Leadbeater, B. J., Gladstone, E., Yeung Thompson, R. S., Sukhawathanakul, P., & Desjardins, T. (2012). Getting started: Assimilatory process of uptake of mental health promotion and primary prevention programmes in elementary schools. Advances in School Mental Health Promotion, 5(4), 258-276.
Leahy, M., & Robb, C. (2013). Building a better school environment for youth with mental health and addiction issues. Toronto, ON: Children’s Mental Health Ontario.
LeBlanc, J. C., Parkington, K., Varatharasan, N., Donato, A., & Bilsbury, T. (2013). Social and emotional learning programs for schools. CPSC Atlantic.
Levitt, J. M., Saka, N., Hunter Romanelli, L., & Hoagwood, K. (2007). Early identification of mental health problems in schools: The status of instrumentation. Journal of School Psychology, 45(2), 163-191. doi:http://dx.doi.org/10.1016/j.jsp.2006.11.005
Manion, I., Short, K. H., & Ferguson, B. (2013). A snapshot of school-based mental health and substance abuse in Canada: Where we are and where it leads us. Canadian Journal of School Psychology, 28(1), 119-135.
Mental Health Commission of Canada. (2012). Changing directions, changing lives: The mental health strategy for Canada. Calgary, AB: Author.
Morrison, W., Kirby, P., & Joint Consortium for School Health. (2010). Schools as a setting for promoting positive mental health: Better practices and perspectives (literature review). Charlottetown, PE: Joint Consortium for School Health
Morrison, W., Kirby, P., & Joint Consortium for School Health. (2010). Schools as a setting for promoting positive mental health: Better practices and perspectives. Charlottetown, PE: Joint Consortium for School Health.
O’Mara, L., & Lind, C. (2013). What do we know about school mental health promotion programmes for children and youth? Advances in School Mental Health Promotion, 6(3), 203-224.
Omstead, D., Canales, C., Perry, R., Dutton, K., Morrison, C., & Hawe, P. (2009). Learning from turbulent, real-world practice: Insights from a whole-school mental health promotion project. Advances in School Mental Health Promotion, 2(2), 5-16.
Paglia-Boak, A., Adlaf, E. M., Hamilton, H. A., Beitchman, J. H., Wolfe, D., & Mann, R. E. (2012). The mental health and well-being of Ontario students 1991-2011: Detailed OSDUHS findings. (CAMH Research Document Series No. 34). Toronto: ON: Centre for Addiction and Mental Health.
Santor, D., & Bagnell, A. L. (2008). Enhancing the effectiveness and sustainability of school-based mental health programs: Maximizing program participation, knowledge uptake and ongoing evaluation using internet-based resources. Advances in School Mental Health Promotion, 1(2), 17-28.
Santor, D., & Bagnell, A. L. (2012). Maximizing the uptake and sustainability of school-based mental health programs: Commercializing knowledge. Child and Adolescent Psychiatric Clinics of North America, 21(1), 81-92.
Santor, D., Short, K., & Ferguson, B. (2009). Taking mental health to school: A policy-oriented paper on school-based mental health for Ontario. Ottawa, ON: The Provincial Centre of Excellence for Child and Youth Mental Health at CHEO.
School-Based Mental Health and Substance Abuse (SBMHSA) Consortium. (2013). School-based mental health in Canada: A final report. Mental Health Commission of Canada.
Tilleczek, K., & Lezeu, K. (in press). Journeys in Youth Mental Health. Education Canada
Ttofi, M. M., & Farrington, D. P. (2011). Effectiveness of school-based programs to reduce bullying: A systematic and meta-analytic review. Journal of Experimental Criminology, 7(1), 27-56.
Wei, Y., Kutcher, S., & Szumilas, M. (2011). Comprehensive school mental health: An integrated “School-based pathway to care” model for Canadian secondary schools. McGill Journal of Education, 46(2), 213-229.
Weist, M. D., & Murray, M. (2008). Advancing school mental health promotion globally. Advances in School Mental Health Promotion, 1(sup1), 2-12.
Wells, G., Biewener, M., Whitman, C. V., Sebian, J., Popp, J., Short, K., . . . Weist, M. D. (2011). The formation of a Canada-United States school mental health alliance. Advances in School Mental Health Promotion, 4(3), 42-54.
-
Journeys in Youth Mental Health
Comments Off on Journeys in Youth Mental HealthYoung people with mental health challenges are among our most vulnerable students in Canada. They are also among our most interesting and courageous. Their lives can be difficult and are too often stigmatized, even though so many are working hard to change this. Many of these young people are navigating a sea of additional troubles such as poverty, loneliness, marginalization, fear and frustration that lead to the spirals of decline[1] and cultures of silence[2] that they have so eloquently detailed for us.
We know a lot about the alarming trends in mental illness in the lives of modern Canadian youth. The Canadian Mental Health Association[3] now estimates that 10-20 percent of Canadian youth are affected by a mental illness, with 3.2 million (12-19 years) at risk for developing depression. Others estimate that 30 percent of students suffer from psychological distress[4] with only a minority (1 in 5) receiving formal supports, which suggests why Canada’s youth suicide rate is now the third highest in the industrial world.[5] We also know that the growth in social inequality and poverty are closely related to mental health for youth.[6] In fact, youth from impoverished backgrounds are three times more likely than their wealthier peers to experience mental health challenges. The most pressing factors in poor mental health include poverty, learning difficulties, abuse/neglect, isolation, lack of support, and lack of access to quality health care and education.[7] However, we know far less about the journeys that these young people are taking toward better mental health.
Journeys: knowing young lives
I knew that it wasn’t just being depressed for a few days, but for a long period of time being depressed… everyone says that getting help is easy, but it really isn’t, like when you get help, you have to wait so many months to actually get the help. So I just feel like nobody does anything for those few months while you’re waiting, and that’s what people really need to do.
And when I went to my cousin, because I could trust her, and tell her I was depressed, she said, ‘What do you have to be depressed about?’ and that’s so depressing, because it’s like, do you not realize that being 16 is hard?
Few researchers and educators have yet had the opportunity to focus on the journeys and experiences of these remarkable young people. Most research illustrates the important, if paradoxical, processes of diagnosis and treatment. But too few young people receive either, and diagnoses can also lead to labeling and further stigmatization. Moreover, what awaits too many kids and families is a heartbreaking experience with a youth mental health system that is fractured and ruptured.
Where have these kids been and where are they going? As educators and parents, this is our shared concern. How do we best assist in the life journeys of these young people? Mapping the journeys of young people into and out of mental health care is one good way of seeing the complexity of these young lives and the best ways to help. Journey mapping is a newer approach to research that gathers stories from youth relating to their experiences and provides visual maps of how they have navigated the system. This strategy is now used by international researchers to identify barriers and facilitators in access and care for mental health.
Our systematic review of this international research literature on journeys in youth mental health yielded 25 recently published English-language journal articles from Canada, Italy, Eastern Europe, New Zealand, the U.S., the U.K., India and China. Three themes arose in our synthesis of this literature:
1. youth journeys in mental health are non-linear in character;
2. barriers and facilitators exist at personal and systemic levels and often in paradoxical fashion; and
3. schools and teachers are crucial in this journey.
Young people take individualized and dynamic journeys to seeking mental health supports.[8] These journeys often start long before they receive formal care from a primary health care provider and with their own early experiences and interactions at home and in school.[9] The non-linear character of these journeys shows us where we could best intervene in a too-often fractured system. We can see in the visual maps how the elements of the system become tied together in a back-and-forth motion as youth and families move in and out of primary health care, school supports, acute health care, and so forth. The recent work in patient journey mapping from Kamloops, B.C.[10] offers an excellent illustration of the journey, with long-term wait times and breaks in the continuity of care. We have further developed this model to assemble a journey map that represents lessons and themes found in our review of literature (see illustrations 1 to 4).
Our image shows the paradoxical journey model that we have detected and demonstrates how personal relationships and systemic structures encountered by youth can exacerbate or alleviate problems that accompany mental health challenges. For example, while there is a shortage of skilled mental health professionals in some areas, most work very hard on a daily basis to go above and beyond their job descriptions in providing excellent care despite the heavy loads. Another example of the paradox is that while poverty stretches the resources and time of these families, many parents are going to extraordinary lengths to advocate for their children in the face of great adversity. Thus, mirror-image supports exist for each barrier, as evidenced in a surprising range of facilitators from which we must launch meaningful change for these young people. Teachers, parents, friends and mental health professionals could form a core community of helpers.
Notably, young people also identify their schools as significant in their journey. In some cases, the school is not seen as a safe or supportive place to be and/or to seek advice or information. School peers are identified as “silent actors” in the journey, with a role that remains both unclear and complex. The role of school peers in inciting stigmatization is clear; however there are also signs of school peers acting in supportive and assistive roles. There is a need for schools to do better in providing these safe spaces for knowledge about mental health.[11]
“Taking mental health to school”
With the complexity and nonlinearity of the youth journeys in mental health, we must ask if and how the school can best provide a reasonable space for prevention and assistance. When youth arrive at school each day, they enter the halls and classrooms with the lives they are immersed in. These lives collide with the range of human and structural relationships that make up the everyday spaces of school. We know that these students are asking for early and local access to mental health supports, a place where they belong without stigma, and a school environment that will both increase mental health awareness and decrease stigma.
An important Canadian study was recently released from the Centre of Excellence of Child and Youth Mental Health in Ontario in which the authors provide an overview of the best ways we can “take mental health to school.” The evidence shows how schools are both necessary and helpful in addressing youth mental health. Not surprisingly, the report finds that “student mental health needs exceed the current capacity of school systems to respond adequately. Education leaders are looking for: leadership and coordination, professional development, and guidance in selecting programs and models of cross-sectoral service delivery…”[12] Programs found to be of use in schools relate to stress or anger management, reducing violence and substance abuse, and modifying the school environment to promote self-awareness and positive relationships. School boards were directed to implement such programs with fidelity and in collaboration with local mental health agencies and parents.
In our recent project on mental health in schools, the investigative team from the Hospital for Sick Children and University of Prince Edward Island took the pulse of students and educators regarding mental health literacy.[13] Working with a mural created by eight young people who experienced mental illness, we installed their original image in six secondary schools in Ontario and four in P.E.I., to invoke a conversation about mental health literacy (see photo on page 4). The image has now been viewed by approximately 7,000 students and teachers in Canada who have shared with us a meaningful conversation about mental health and stigma. The installation of the mural was somewhat different in each school, with many young people and teachers assisting us in finding a prominent place for it to hang and acting as ambassadors for the mural during the two weeks of installation in each school. The installation was followed by a large group “talk back” session in the form of an assembly in which the Canadian Mental Health Association joined us in leading a session about the mural and about youth mental health. This was followed by focus group conversations with students and educators (separately) and by analysis of the writings and comments they provided on large sheets of paper and comment cards left for this purpose.
Early analysis of the data from P.E.I. schools suggests that the majority of students and educators were grateful for the opportunity to have a mental health conversation. To many, it seemed long overdue. They also commended the young artists for their demonstration of great courage in sharing their mental health journeys in artistic form. In fact, some of these schools have now taken on similar art-inspired projects with their own students for Mental Health Awareness Week. The students appreciated the use of art in depicting the complex experiences of young people in mental health, as they felt that it allows for deeper understanding and interpretation of the experiences they are facing. Many students also expressed that the mural and conversation in the school provided reassurance that they were not alone in their mental health experiences. They reported a clear desire to learn more about youth mental health and illness. Students wanted the opportunity to have further discussions, learn about the clinical aspects of mental health and illness, and better understand what services are available to them in school and community. They expressed a strong need to better address and eliminate stigma in their schools and communities.
I think the mural spoke of issues that people struggle with. I think the best ways to get knowledge are by having small meetings and discussing it to give everyone the chance to speak in a small group. I think art is a beautiful and approachable way to discuss and get knowledge on mental health. – student
The thing for me is that, I am not trained in that [mental health support]. We are talking about kids, but let’s face it, there are teachers and adults in the community who have all these issues… And my curriculum doesn’t really allow for a broad conversation, right? So I see the mural as a stimulator of mental health discussion and it shows the point of having the conversation, and how we keep that going.” – educator
Our review of the literature and our interviews with students and teachers in the mural project uphold important messages about youth journeys in mental health. We contend that Canada is moving along a good path in addressing the alarming trends in youth mental health. We offer youth journeys as a tremendous jumping-off point in examining the complexity of these young lives and in pointing to promising ways to support them. There is need to better coordinate services, reduce wait times, meaningfully address stigma and open up new spaces for families, schools, and mental health professionals to assist youth in their journeys to mental health. Their experiences call us to action in breaking the spirals of decline and cultures of silence that society has left them to negotiate.
Next Steps
We are pleased to announce ACCESS-MH,[14] a five-year project in Atlantic Canada, funded by the Canadian Institutes of Health Research. Our study applies youth mental health journeys with related statistical information from Prince Edward Island, Newfoundland, New Brunswick and Nova Scotia. Building upon the knowledge and methods now emerging in youth mental health journeys, this project includes conversations with parents, teachers, primary health care providers, and community members. We also invoke arts-based methods of understanding experiences and mapping journeys. The variety of participants will further identify complex problems youth face in seeking mental health care. Our work aims to better assist in the creation of a more coherent network of support and programming for our vulnerable and courageous Canadian youth.
Photo: Katherine Boydell
First published in Education Canada, March 2014
EN BREF – La santé mentale des jeunes est une préoccupation de taille de la société et des écoles canadiennes. En fait, il s’agit d’une question dont on parle de plus en plus dans le monde entier. Ce texte présente une nouvelle façon prometteuse de comprendre le problème en plaçant les parcours de vie des jeunes au centre de notre attention. Nous ouvrons ainsi de nouveaux espaces où les écoles peuvent collaborer avec des partenaires de la collectivité et du domaine médical de la santé mentale pour constituer un système plus cohérent destiné à entourer la vie complexe et courageuse de nos élèves.
[1] K. Tilleczek and V. Campbell, “Barriers to Youth Literacy: Sociological and Canadian insights,” Language and Literacy 15, no. 2 (2013): 77-100.
[2] S. Kutcher and A. McLuckie, Evergreen: A child and youth mental health framework for Canada, for the Child and Youth Advisory Committee, Mental Health Commission of Canada (Calgary: 2010).
[3] Canadian Mental Health Association, Fast Facts About Mental Illness. www.cmha.ca/media/fast-facts-about-mental-illness/#.Us1uj7SmYk8
[4] A. Paglia-Boak, R. E. Mann, E. M. Adlaf, J. H. Beitchman, D. Wolfe, and J. Rehm, The Mental Health and Well-being of Ontario Students 1991–2009: Detailed OSDUHS findings (Toronto: Centre for Addiction and Mental Health, 2010).
[5] E. J. Costello, H. Egger, and A. Angold, “10-year Research Update Review: The epidemiology of child and adolescent psychiatric disorders: Methods and public health burden,” Journal of the American Academy of Child and Adolescent Psychiatry 44, no. 10 (2005): 972–986; CMHA, Fast Facts, www.cmha.ca/media/fast-facts-about-mental-illness/#.Us1uj7SmYk8
[6] For a current review of literature linking social inequality, poverty and mental health see Tilleczek, Ferguson, Campbell and Lezeu (in press), “Mental Health and Poverty in Young Lives: Intersections and directions,” Canadian Journal of Community Mental Health.
[7] E. L. Lipman and M. Boyle, Linking Poverty and Mental Health: A lifespan view (Ottawa: The Provincial Centre of Excellence for Child and Youth Mental Health at CHEO, 2008).
[8] K. Boydell, R. Pong, T. Volpe, K. Tilleczek, E. Wilson, and S. Lemieux, “Family Perspectives on Pathways to Mental Health Care for Children and Youth in Rural Communities,” Journal of Rural Health 21, no. 2 (2006): 182-188.
[9] S. De la Rie, G. Noordendos, M. Donker, and E. van Furth, “Evaluating the Treatment of Eating Disorders from the Patient’s Perspectives,” International Journal of Eating Disorders 39, no. 8 (2006): 667-676.
[10] S. Scott, S. Sze, K. Weatherman, and R. Gorospe, “Kamloops Patient Journey Mapping Report, Child and Youth Mental Health” (unpublished manuscript, 2013).
[11] K. M. Boydell, T. Volpe, B. M. Gladstone, E. Stasiulis, and J. Addington, “Youth at Ultra High Risk for Psychosis: Using the Revised Network Episode Model to examine pathways to mental health care,” Early Intervention In Psychiatry 7, no. 2 (2013): 170-186.
[12] D. Santor, K. Short, and B. Ferguson, Taking Mental Health to School: A policy-oriented paper on school-based mental health for Ontario (Ottawa: The Provincial Centre of Excellence for Child and Youth Mental Health at CHEO, 2009), 6.
[13] K. Boydell, “Using Visual Arts to Enhance Mental Health Literacy in Schools,” in Youth, Education and Marginality: Local and global expressions, eds. K. Tilleczek and B. Ferguson (Waterloo: Wilfrid Laurier University Press, 2013).
[14] Atlantic Canada Children’s Effective Service Strategies in Mental Health is a CIHR-funded project lead by Dr. Rick Audus (MUN), Dr. Kate Tilleczek (UPEI), Dr. Scott Ronis (UNB) and Dr. Micheal Zhang (SMU).
-
School Overload
Comments Off on School OverloadOver the past 60 years, our society has moved evermore toward a school-centric view of child development, which I’m calling here the schoolish view. The schoolish view is this: Children need regular adult guidance. Children benefit more when they are supervised and directed by adults than when they play on their own. Children, including adolescents, have immature brains and are ill equipped to make good decisions for themselves. Left to their own devices they will take risks and ignore dangers, so it is best to monitor them continuously. Learning derives mainly from school lessons and other adult-directed activities, not from children’s self-directed activities. Parents should be assistant teachers. They should monitor their children’s homework, reward their children for doing well in school, seek “teachable moments,” buy toys that are specifically designed to teach the kinds of skills and information emphasized in school, and encourage their children to join school-like, adult-directed sports, clubs, and classes outside of school.
There are many reasons for the rise of this schoolish view, but we educators are at least partly to blame. We have allowed school to become more central to children’s lives (and to their parents’ lives) than it should be. We have forgotten that the most important lessons children must learn in order to grow into socially and psychologically competent adults are not taught in school, but are learned through self-directed activities, especially play. Here I will summarize some of the evidence for the damage that the schoolish view has done and offer some hints as to how we might help restore children’s freedom to play.
Young parents and teachers may not even realize the degree to which our culture has shifted in its view of childhood. When I was a child, in the 1950s, school had not yet burst out of its walls to affect the child’s whole world. The school day was six hours long, as it generally is today, but in the elementary schools I attended we had a half-hour recess in the morning, a full hour of free time at lunch, and another half-hour recess in the afternoon. At lunch we were free to go anywhere we wanted, including off campus.
Homework for elementary school students was almost unheard of. Out of school, most of us had some chores, and some had a part-time job (such as delivering newspapers, mowing lawns, or babysitting), but even that gave us a sense of personal accomplishment, self-direction, and maturity that is rarely found in schoolwork. The rest of our time, including all summer long, was largely our own, to do with what we wanted. We were free to go where we wanted, as long as we could get there on our own.
If we played sports, they were almost always pickup games, where we had to negotiate the rules and solve all problems ourselves, without adult coaches or umpires to tell us what to do. Our hobbies were of our own choosing and under our own control. In the summer we read what we wanted, not assignments from a school-dictated reading list. There seemed to be a general understanding, not necessarily stated, that children need lots of time to play and explore on their own for healthy development.
These are not just nostalgic musings. Social scientists have documented the continuous and dramatic decline of freedom of movement and play for children over these decades.[1] The historian Howard Chudacoff refers to the first half of the 20th century as “the golden age” of free play for children in the United States.[2] But since about 1955, adults have continuously chipped away at children’s freedom, as the schoolish view has gained ever-greater momentum.
As children’s freedom has declined, we have seen a gradual, but ultimately huge, increase in all sorts of mental disorders in children and young adults. These have been documented by analyzing the results of clinical assessment questionnaires given in unchanged form to normative samples of young people over the decades.[3] (The findings I describe here are from the U.S., where the most extensive studies have been done, but there is reason to believe that the same applies generally to Canada, the UK, and other Western countries.) By these measures, the rates of clinically serious depression and anxiety in young people increased five- to eight-fold between the mid 1950s and late 1990s.[4] During that same period, the suicide rate quadrupled in children under 15 and more than doubled in young people between 15 and 24 (and did not increase in older adults).[5] More recently, the rates of childhood depression and suicide, and some indices of anxiety, have leveled off or even declined somewhat, but these recent changes appear to be attributable to a huge increase in the prescription of psychoactive drugs to young people and to suicide-prevention programs, not to a cultural shift that has made children’s lives less depressing or anxiety-inducing.[6]
Analyses of other clinical questionnaires given over the years to normative samples of children and adolescents have produced similarly sad results. Such research reveals that young peoples’ sense of being in control of their own lives has been declining continuously since the 1950s,[7] that narcissism has been increasing and empathy decreasing ever since tests for these were developed in the late 1970s,[8] and that creative thinking has been declining in K-12 schoolchildren, at least since the mid 1980s.[9]
What has caused this deterioration in children’s mental and social well-being? The changes do not correlate with economic cycles, or wars, or with changes in the divorce rate, but do correlate very well with the decline in children’s freedom. In fact, these are exactly the changes that we would predict would occur as a result of a decline in children’s opportunities to play freely.[10]
In play, children discover and pursue their passions, with no bells interrupting them, and develop skills related to those passions, which can lead eventually to rewarding and enjoyable careers. In play, away from adults, children learn to solve their own problems and take control of their own lives. In social play, children learn how to make friends and see from one another’s perspectives. Play, by definition, is an activity that you are always free to quit; so, to keep any game going, each player must be concerned with the other players’ happiness, so they don’t quit. To do that, each player must see from the other players’ points of view, which is the essence of empathy and the opposite of narcissism.
Play builds emotional resilience that protects children from clinically significant depression and anxiety. In play children develop confidence that they can solve problems as they arise, so the world become less frightening and more manageable. When children play at “dangerous” things, such as climbing high in trees, they are testing and building on their own capacity to experience and overcome fear – a capacity that allows them to experience fear without panic, which may one day, in a real emergency, save their lives. Young mammals of many species also play at moderately dangerous activities, apparently for the same reason.[11] Children also inevitably, on occasion, get angry at one another in their play, but if they are to continue playing they must learn to control that anger. And so, in play, children learn to regulate their emotions. They learn to take life’s stressors with equanimity.
When adults are always around to solve children’s problems, resolve their disputes, and stop them from playing in ways that look rough or dangerous, children can’t learn these things. Adults, of course, are crucial to children’s well-being. They are models, nurturers, sources of security, and teachers. But when adults take over children’s lives as completely as they do now, the results are harmful. Play, away from adults, is how children learn to become adults, because that is where they must be responsible for themselves and for one another. We need to permit children lots of opportunity for such play if we want them to grow up socially competent, emotionally resilient, and happy.
We educators can help children by doing the opposite of what so many of us are doing now. We can advocate for less time sitting in classrooms, less homework, less pressure to pass tests or take honours courses or get high grades, and more opportunity for free play and exploration with no adults hovering. We can open up school playgrounds and gymnasiums and art rooms for free play after school hours, perhaps with a teenaged or adult supervisor present just for emergencies, not to intervene or interfere. We can work to reduce, rather than increase, parents’ concerns about their children’s school performance. We can help parents and others in the community realize that education is far more than schooling. It is all of learning, and most of what children must learn for a happy and healthy life can occur only outside of the classroom, when children are truly free. We can help our communities realize that safe places for children to play with one another are at least as important as good schools, and we can work in our communities to create those safe places.
Photo: iStock
First published in Education Canada, March 2014
EN BREF: Depuis plus d’un demi-siècle, notre société évolue de plus en plus vers ce que l’auteur appelle une approche « scolarisante » de l’éducation des enfants, qui sont pratiquement toujours surveillés et dirigés par des adultes et où le jeu libre tient très peu de place. Cette diminution de la liberté pendant l’enfance s’est accompagnée de hausses marquées de la dépression, de l’anxiété, du sentiment d’impuissance et du suicide, de même que d’une baisse de l’empathie chez les jeunes. L’auteur soutient que ces déclins du bien-être mental et social correspondent exactement à ce qu’on devrait s’attendre par suite d’un déficit de jeu et d’autres possibilités d’autodétermination. Il attribue aux éducateurs, du moins en partie, la responsabilité de ces changements sociétaux et nous incite maintenant à faire ce que nous pouvons pour les renverser.
[1] Peter Gray, “The Decline of Play and the Rise of Psychopathology in Children and Adolescents,” American Journal of Play 3, No. 4 (2011): 443-463.
[2] Howard P. Chudacoff, Children at Play: An American history (New York: New York University Press, 2007).
[3] Gray, “The Decline of Play,” 443-463.
[4] Jean M. Twenge, “The Age of Anxiety? The birth cohort change in anxiety and neuroticism, 1952-1993,” Journal of Personality and Social Psychology 79, No. 6 (2000): 1007–21; Jean M. Twenge, Brittany Gentile, C. Nathan DeWall, Debbie Ma, Katharine Lacefield, and David R. Schurtz, “Birth Cohort Increases in Psychopathology Among Young Americans, 1938–2007: A cross-temporal meta-analysis of the MMPI,” Clinical Psychology Review 30, No. 2 (2010): 145–54.
[5] For suicide rates by age group from 1950 to 2005, see: www.infoplease.com/ipa/A0779940.html#axzz0zVy5PKaL
[6] Jean M. Twenge, “Generational Differences in Mental Health: Are children and adolescents suffering more, or less?” American Journal of Orthopsychiatry 81, No. 4 (2011): 469-472.
[7] Jean M. Twenge, Liqing Zhang, and Charles Im, “It’s Beyond My Control: A cross-temporal meta-analysis of increasing externality in locus of control, 1960–2002,” Personality and Social Psychology Review 8, No. 3 (2004): 308–19.
[8] Sarah H. Konrath, Edward H. O’Brien, and Courtney Hsing, “Changes in Dispositional Empathy in American College Students over Time,” Personality and Social Psychology Review 15, No. 2 (2011): 180-198; Jean M. Twenge, “The Evidence for Generation Me and Against Generation We,” Emerging Adulthood 1 (2013): 11-16.
[9] Kyung Hee Kim, “The Creativity Crisis: The decrease in creative thinking scores on the Torrance Tests of Creative Thinking,” Creativity Research Journal 23, No. 4 (2011): 285-295.
[10] Peter Gray, Free to Learn: Why unleashing the instinct to play will make our children happier, more self-reliant, and better students for life (New York: Basic Books, 2011).
[11] Marek Spinka, Ruth C. Newberry, and Marc Bekoff, “Mammalian Play: Training for the unexpected,” Quarterly Review of Biology 76, No. 2 (2001): 141–68.
-
Minding Your Mind
Comments Off on Minding Your MindRecently, in Canada and indeed globally, the unmet emotional and mental health needs of young people stand squarely in the spotlight. Many young people navigate the changes of adolescence well, yet some experience serious difficulty. Mental health problems such as anxiety and mood disorders, psychosis, eating disorders, personality disorders and substance abuse begin in childhood, during peaks in brain development and impacted by complex social contexts.[1] One in five Canadian youth is at risk for a mental illness,[2] while only 25 percent of youth get the help they need, in the way they need it.[3]
Stigma is a massive barrier for youth experiencing mental health challenges. It contributes to feelings of shame for being different and perpetuates silence. A young adult describes the burden of stigma during her extended high school experience: “You don’t know how to tell them (peers) and it’s not something they can visibly see is wrong with you… I wish I could go back now, stand in front of my class and just say, Hi I’m Paige and I have an anxiety disorder and that’s that.” Instead of finding support from her peers, she tackled completing high school – something that felt impossible – alone.
Removing the barriers of stigma requires increased understanding and improved recognition of mental health problems, and this can begin in the classroom by incorporating mental health content. A recent Canadian study found that older teens and young adults are most inclined to self-manage or seek support from friends or family before accessing more formal, traditional interventions for mental health care.[4] To support self-care, it is essential for adults and youth to be equipped with knowledge and resources to draw upon in their daily lives.
mindyourmind
Building this knowledge base early is one of the goals of mindyourmind, a not-for-profit program funded in part by the Ontario Ministry of Health and Long Term Care. The program recognizes that young people want credible information and provides a 24-hour-a day space – through a website and social media platforms – where youth can seek out resources about mental health that appeal to them. Resources on the website, designed to reduce the stigma associated with mental illness and increase access and use of both professional and peer-based support, are created in collaboration with youth. This partnership ensures that resources resonate with the user. By engaging youth in mental health promotion online and in person, mindyourmind promotes relevant mental health awareness and inspires youth to act, to “reach out, get help and give help” during difficult times.
Community partnerships
Responding to the need for resources, Learning Coordinators in the Thames Valley District School Board (TVDSB) in Southwestern Ontario approached mindyourmind to develop resources for Grade 11 Physical Health Education and Grade 9/10 Guidance and Learning Strategies. Over several brainstorming sessions, mindyourmind’s clinical and educational staff and TVDSB Learning Coordinators collaborated on the outlines of the “Minding Your Mind” lessons. The lessons are based on Ministry expectations and the unique needs of the TVDSB’s populations, and reflect a comprehensive view of mental health rather than solely a bio-medical model. A teacher’s guide is included in the lessons, which offers class discussion primers and activity extension suggestions.
The team decided on digital formats because it allowed for student-directed units and for information to be presented using multiple delivery methods, appealing to a variety of learning styles and differentiated learning. Existing interactive digital tools, previously created by mindyourmind’s youth-adult teams during intensive “charette” or design workshops, were integrated into the outlines of written content to provide different representations of facts about mental health. These tools and other resources find a permanent home on the mindyourmind website in addition to being used in other resources. One of the interactive tools in the Grade 11 lessons, “The Anatomy of a Panic Attack,” was co-developed earlier by a group of 10 youth aged 15-24 from across Canada and describes what a panic attack looks and feels like while offering suggestions on coping.
Existing and custom-created videos of youth discussing mental health issues provide concise information, and personal stories written by young people convey an authenticity that learners can identify with and learn from, allowing for reflection and a transfer of knowledge between youth.
Once the technical and graphic design team added their expertise, field-testing began. As part of testing, Learning Coordinators facilitated meetings between mindyourmind and TVDSB department heads, where lesson delivery was demonstrated. Questions were addressed and then feedback from classroom surveys was collected. During this phase, the Mental Health Commission of Canada[5] put out an offer to evaluate existing programs that aimed to reduce stigma in youth, and an evaluation of the Grade 11 Minding Your Mind lessons was accepted.
Evaluation of the Grade 11 lessons on stigma reduction
As part of the MHCC evaluation, Dr. Heather Stuart’s research team at Queen’s University found that the students’ attitudes moved toward understanding that the course of a mental illness is not entirely in one’s control. One student responded, “… it (having a mental illness) doesn’t make them any less than you.” Beliefs about the potential for recovery from a mental illness were shifted positively. The most positive shift for students occurred in a category focusing on unpredictability and social distance. Questions about unpredictability addressed the myth that all people with mental illnesses are unreliable or unpredictable. Questions about social distance asked about a person’s comfort with being a classmate with or even dating someone with a mental illness. A student responded, “They are normal people too and deserve respect.” Attitudes also changed around valuing socially responsible actions such as volunteering with a program that benefits people with a mental illness.
The changes in stigma and the increased social tolerance in student responses as a result of the Minding Your Minds lessons showed that this digital approach was effective. Together with the TVDSB Research Manager, mindyourmind co-presented preliminary evaluation results to the TVDSB Mental Health and Wellness Committee and then participated as Youth Team Advisors in the five-year School-Based Strategic Mental Health Plan.
In the classroom
Many positive responses indicated that the students enjoyed the delivery of the lessons. In a computer lab, students access and use the modules in either a self-directed or guided way, depending on teacher preference, to learn about and practice increased self-awareness through goal-setting, decision-making, and interpersonal skill building. Students explore the positive and negative effects of stress, describe the influence of mental health on overall well-being, and encounter personal stories about young people dealing with mental health issues ranging from everyday stress all the way to specific illnesses such as anxiety and schizophrenia.
The digital format is designed to meet youth “where they are,” in terms of readiness and learning preferences. Students determine the speed of learning and return to previously viewed materials, encouraging self-regulation and responsibility. Assessment for and as learning are dispersed throughout units, prompting learners to reflect and to review where necessary. Evaluations are differentiated based on learning preferences, allowing students to work to their strengths to demonstrate learning.
Students taking next steps
Using a format that builds on the pillars of youth culture (e.g. music, fashion, technology, art, sports), the modules scaffold learning about mental health in relatable, relevant and practical ways using materials co-created by their peers. Students are better informed about mental health issues and know where to go later if and when information is needed for themselves or for friends. Lessons introduce students to resources in the community as well as mindyourmind’s website. Through the lessons, students see the positive results of their peers’ volunteering in the community. At the end of the lessons, students are invited to initiate activities and get involved in their own personal networks, schools or wider communities to make change.
The most effective change happens when youth, educational teams and community partners work together. In order to engage youth in the discussion, we need to start where they are, using ever-changing youth culture as an entry point for partnerships and in the classroom to participate in dialogues that concern their health, and to build the capacity to reach out, get help give help.
Photo: Ethan Myerson (iStock)
First published in Education Canada, March 2014
EN BREF – L’amélioration des connaissances en santé mentale constitue une façon essentielle de répondre aux besoins non comblés des jeunes en matière de santé mentale. Les jeunes, les équipes pédagogiques et les partenaires communautaires peuvent travailler ensemble pour réduire la stigmatisation et habiliter les enseignants et les jeunes. Grâce à un partenariat entre mindyourmind, un organisme communautaire axé sur l’engagement des jeunes, et le conseil scolaire local, des leçons numériques ont été instaurées en 9e, 10e et 11e années. Une évaluation réalisée par l’initiative « Changer les mentalités » de la Commission de la santé mentale du Canada a constaté des changements en matière de stigmatisation et une tolérance sociale accrue dans les réactions des jeunes par suite des leçons, indiquant que l’approche fonctionne.
[1] T. Paus, M. Keshavan and J. N. Giedd, “Why do many psychiatric disorders emerge during adolescence?” Nature Reviews Neuroscience 9, No. 12 (2008): 947-957.
[2] Canadian Psychiatric Association, Youth and Mental Illness (2013). http://publications.cpa-apc.org/browse/documents/20
[3] Statistics Canada, Canadian Community Health Survey: Mental health and well being (2002). www.statcan.gc.ca/daily-quotidien/030903/dq030903a-eng.htm
[4] M. Marcus and H. Westra, H., “Mental Health Literacy in Canadian Young Adults: Results of a national survey,” Canadian Journal of Community Mental Health 31, no. 1 (2012): 1-15.
[5] Mental Health Commission of Canada, Opening Minds. www.mentalhealthcommission.ca/English/initiatives-and-projects/opening-minds?routetoken=4e7e3879325d7eb9d62c51a03176d8ac&terminitial=39
-
Outside the Box
Comments Off on Outside the BoxCan you remember what it felt like to be a kid exploring the natural world? What if that feeling could be brought to school? If children had an opportunity to learn in a natural setting, what could that mean for their academic performance?
A recent Ipsos Reid poll shows that 97 percent of adult Canadians agree that nature is important to their family’s well-being, and 87 percent felt that given the choice, they would prefer to spend family time outdoors in nature, as opposed to indoors. Overall, most of these adults agreed that the more connected they feel to nature, the happier they are. If Canadians – young and old – are indeed happier while in nature, an outdoor classroom initiative could be exactly what’s needed for a generation that often struggles to find a connection to, or even opportunities to explore, nature.
Today, work life and hectic schedules often take precedence over making time for outdoor unstructured play. Moreover, what was once considered safe for youngsters (like heading out on your bike with a buddy for the day) is often now seen as requiring adult supervision. Modern urban life has drastically diminished children’s opportunities to explore nature on their own or with the family, at a time when children need it more than ever.
Author Richard Louv writes of his concern for children, drawing links between lack of exposure to nature and adolescent hardships like obesity, attention disorders and depression. Louv, author of Last Child in the Woods: Saving our children from Nature-Deficit Disorder, advocates early contact with nature and says that it’s our job to pass an appreciation of nature on to our children. He writes, “These are the moments when the world is made whole. In my children’s memories, the adventures we’ve had together in nature will always exist.”[1]
Louv also explores the idea of a nature-based education and what trading classroom walls for shrubbery and sunshine could do for a child’s ability or desire to learn. “An environment-based education movement – at all levels of education – will help students realize that school isn’t supposed to be a polite form of incarceration, but a portal to the wider world,” he notes in his book.[2]
The benefits of spending more time in nature go beyond enjoyment. Major physical and mental health benefits can be attributed to time spent outdoors. Jules Pretty and her colleagues, authors of Nature, Childhood, Health and Life Pathways, found that time in nature can lead to reduced amounts of anxiety and stress and improved self-esteem. Their report looks at three stages of childhood and explores the implications of nature-based experiences within them. The authors found that enhanced experiences in nature can lead to positive behavioural changes, a better connection with the natural world, and an improved ability to learn.[3]
Bringing nature to school
Educators across Canada are taking note of these findings and are taking advantage of local parks and conservation areas to give their students a direct learning experience with nature.
Melissa Anema, from Lord Strathcona Elementary School in Vancouver’s Downtown Eastside, took part in nature-based programming for her Grade 4/5 class. She says her students have few opportunities to experience these natural connections because of their own concerns at home.
“For my students – most of whom struggle with basic issues like having a safe home to go to, having caregivers who are solid and dependable, having enough to eat throughout the day, etc. – learning about and connecting with nature is often very far from their inner-city reality,” Anema says.
Last fall, Anema and her class visited the North Vancouver Outdoor School through the HSBC Bank Canada Nature Days program outside of Squamish, B.C. She and her students waded among salmon in a nearby stream and learned about the species’ life cycle and the integral role it plays in Canadian ecosystems and businesses. “It was so incredible to see students who are so often withdrawn or just opting out of learning jump into learning like never before,” says Anema. “They were really left to think about human impacts on the fish, and why our interventions with the hatchery were necessary. It inspired a lot of thinking and discussion both during and afterwards.”
Time in nature can lead to reduced amounts of anxiety and stress and improved self-esteem.
In Toronto, the Toronto District School Board (TDSB) offers a “beyond the classroom” learning experience through an innovative outdoor enterprise known as Toronto Outdoor Education Schools (TOES). Offered for 11 different school subjects, TOES is available in day and overnight school program centres across the Greater Toronto Area. Both daytime and overnight offerings aim to connect children to the natural world, through a variety of outdoor, curriculum-based activities. One of these TDSB programs, Hillside Outdoor Education School, is located in Rouge Park, Canada’s largest urban park and an ideal setting for this kind of program.
But not all schools or school boards have the on-site resources or capacity to facilitate this kind of program. Some education- and nature-centred organizations have developed programming to help with this. Nature Days, an education initiative created by the Nature Conservancy of Canada (NCC) and Earth Rangers, provides adventures in conservation for school children at sites across the country. This youth-focused program brings Canadian students into nature to work among conservation biologists and learn first-hand how to care for some of the country’s most vulnerable natural areas.
Erica Thompson, Conservation Engagement Coordinator for NCC, highlights the important role that direct observation plays in learning, and notes that actually seeing, smelling and feeling the subjects under study allows children to learn on a whole different level. “Bringing children to nature reserves brings the classroom into the natural world. So learning about forests within a forest habitat, learning about wetlands by standing on the edge of one, and seeing a salamander under a log for the first time – these are the kinds of experiences that we hope inspire lifelong learning and curiosity about the natural world.”
Raymond Martynowski, a teacher at Chine Drive Public School in Scarborough, Ontario, recently attended a Nature Days event with his Grade 3 class and noticed a refreshing thirst for knowledge among his students.
“Our kids are going to be the stewards for our environment, for the future. And if they don’t have a personal connection to it – if they haven’t been out in nature – they don’t really know what they’re preserving and what they’re saving, or why it’s so important,” he says. “It really is amazing to see how excited the kids are just to see a spider in the grass, to touch a millipede, to pick up a leaf and look at the kinds of edges it has – you’d be surprised, you wouldn’t think they would be that excited, but when we’re here, out of the city, walking together, it’s just a different side of the student. It’s really nice to be able to see that.”
Engagement, participation, innovation, inspiration – these “extra-curricular” expectations could arguably be tackled by bringing more nature-based activities and programs to education. We have the tools; we just need to use them… outside.
Find a nature education program near you
Nature and outdoor education programs are offered by a variety of organizations. Here are a few national programs available across the country; you can also check for local programs which may be offered by camps, ecology groups, and conservation areas.
Outward Bound Canada
At OBC the wilderness is the classroom. OBC offers specialized school programs focusing on leadership, technical skills, teamwork and personal development. Each course is designed to teach students about their potential and instil a can-do approach to everything they do.
To learn more, visit outwardbound.ca
The Nature Conservancy of Canada
The NCC, in partnership with Earth Rangers and HSBC Bank Canada, brings classrooms to natural areas to learn about species and habitat conservation work. Led by conservation professionals, children are able to see, firsthand, what it means to preserve natural habitat. The program is available in Vancouver, Calgary, Toronto and Montreal and is generally offered to Grade 4 and 5 classes.
To learn more visit natureconservancy.ca
Forest School Canada
FSC works to connect youth with nature in an academic setting. FSC emphasizes outdoor learning at early, primary and secondary levels of education, and provides a natural setting for engaging, youth-focused learning activities. FSC is currently developing a full-fledged Canadian Forest School, and in the meantime is providing schools across Canada with the outdoor resources and curriculum materials needed to carry its lessons out independently.
To learn more visit forestschoolcanada.ca
Photo: iStock
First published in Education Canada, January 2014
EN BREF – Il existe d’abondantes indications selon lesquelles les enfants d’aujourd’hui sont privés de contact avec la nature et que le temps passé dans un milieu naturel procure une foule d’avantages émotionnels et cognitifs. Bien que l’enseignement en plein air soit souvent éclipsé par la multitude des autres exigences du curriculum, les enseignants qui réussissent à sortir leurs élèves du confinement de leur salle de classe soulignent avec enthousiasme la valeur de l’apprentissage de première main de la nature et de la conservation. À l’aide d’exemples donnés par l’auteur et amateur de nature Richard Louv et d’autres éducateurs canadiens, les auteurs incitent les éducateurs à profiter des ressources et de la programmation liées à la nature qu’offre leur collectivité et à aider leurs élèves à découvrir le milieu naturel.
[1] Richard Louv, Last Child in the Woods: Saving our children from Nature Deficit Disorder (New York: Algonquin Books, 2005), 316.
[2] Richard Louv, Last Child in the Woods, 226.
[3] J. Pretty, C. Angus, M. Bain, et al., Nature, Childhood, Health and Life Pathways (United Kingdom: University of Essex, 2009).
IDEAS TO SUPPORT EDUCATORS : Subscribe to the EdCan e-Newsletter
Quality research, reports, and professional learning opportunities.